The Chemistry of CBD
Cannabidiol (CBD) is a phytocannabinoid compound first described by Adams et al. in a 1940 paper in the Journal of the American Chemical Society.1 Its chemical structure was elucidated in 1963 by Mechoulam and Shvo2 and confirmed in Jones’s x-ray crystallography study in 1977.3 CBD is the most common phytocannabinoid found in hemp plants.4
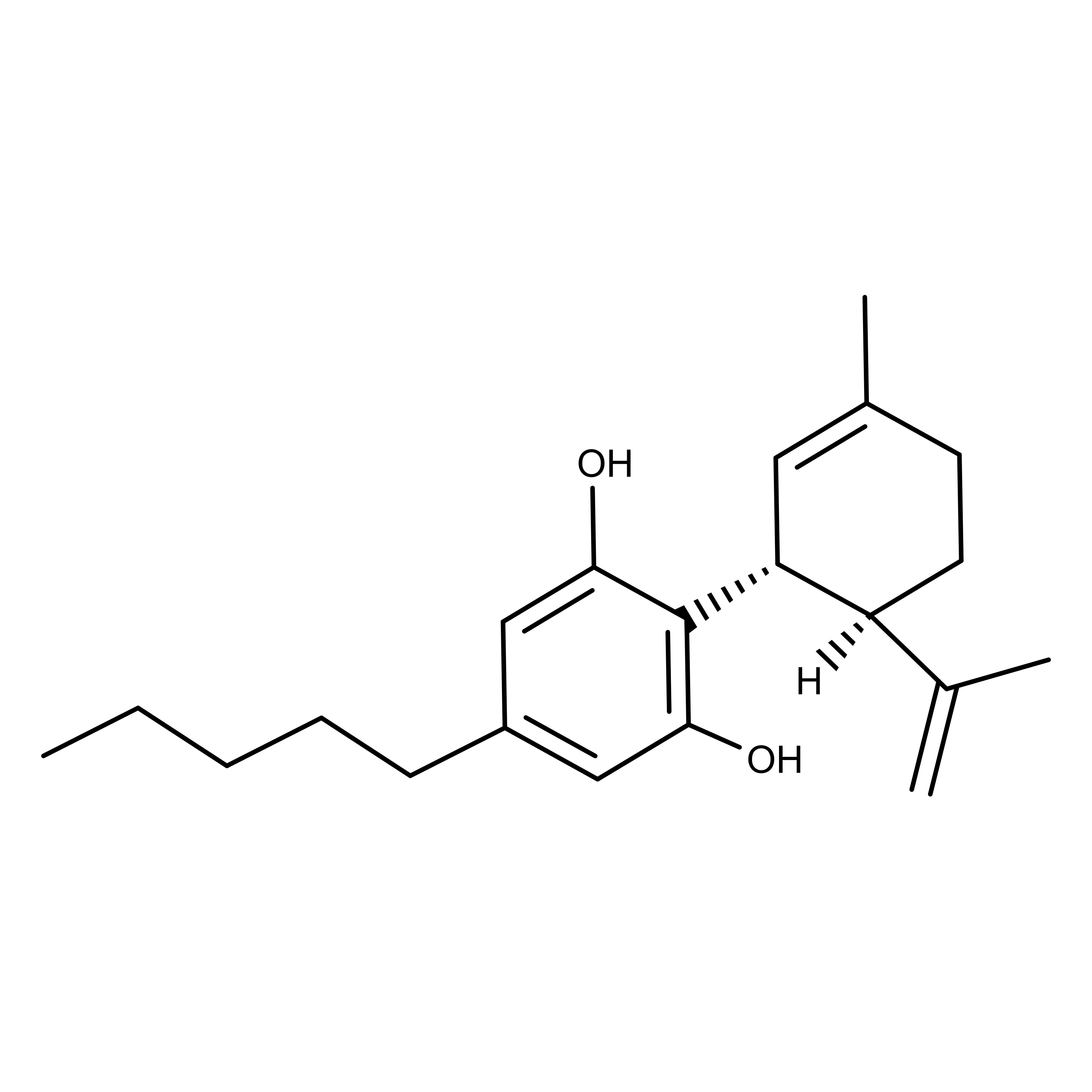
Chemically, CBD is described as a 21-carbon terpenophenolic compound.5 Its synthesis pathway in Cannabis plants begins with the precursors olivetolic acid and geranyl pyrophosphate. With the help of the enzyme CBDA synthase, these compounds are transformed into cannabidiolic acid. Finally, decarboxylation triggered by light, heat, and/or aging causes the conversion to CBD.
The Pharmacology of CBD
A pharmacological study in 1970 indicated that CBD had no ‘cannabis-like’ activity.6 Additional studies early in the decade reported that the effects of CBD did not mimic those of Cannabis in humans7,8 and animals.9 However, in 1970, Carlini et al. hypothesized that CBD could act as an antagonist by stating, “…cannabidiol could counteract Δ9-THC [tetrahydrocannabinol] effects on motor activity in mice.”10 They formed this hypothesis from data obtained during behavior tests in mice using different mixtures of Δ9-THC and CBD.
In 1970, Uliss et al. reported an intravenous (iv) LD50 of 50 mg/kg for CBD in mice.11 They also observed the minimum effective dose (MED) for inducing ataxia was 25 mg/kg iv.
In 1993, Compton et al. observed a Ki of 4,350 nM for CBD at the CB1 (cannabinoid 1) receptor12 (see table at the end of this article). In 1996, Showalter et al. reported a Ki at CB2 of 2,860 nM.13
In a 2019 study, Tham et al. reported on the allosteric modulation effects of CBD in the British Journal of Pharmacology.14 Using receptor models they made, the data showed that CBD was a negative allosteric modulator at CB1 and a partial agonist at CB2.
They also tested a compound with a nearly identical chemical structure, but which has different pharmacological properties, (-)-cannabidiol-dimethylheptyl (CBD-DMH). This compound showed mixed agonist/positive allosteric modulation at CB1. At CB2 it was “a partial allosteric modulator of cAMP [cyclic AMP] modulation but a negative allosteric modulator of ß-arrestin 1 recruitment.” The authors suggested that the different behaviors of these two compounds “may explain their in vivo effects and illuminates the difficulties associated with the development of allosteric modulators for CB1 and CB2 receptors.”
A 2011 review paper by Russo summarized the entourage effects between CBD and terpenoid compounds also found in Cannabis including limonene, linalool, and pinene.4
In 2019, Morrison et al. reported that their experiments showed CBD promoted bidirectional drug-drug interactions (DDI) when co-administered with other drugs including clobazam, a benzodiazepine used to treat epilepsy.15 The risk posed by the DDI with clobazam was not the drugs themselves, but the increased amounts of their metabolites that were generated in the body. Interestingly, CBD is known to affect voltage-gated sodium ion channels in cells which are thought to be involved in fatal forms of epilepsy and chronic pain.16,17
The Applications and Potential of CBD
In a 2020 critical review paper in the Journal of Medicinal Chemistry, Nelson et al. commented on the challenges of understanding the beneficial effects of CBD, and why some researchers are pivoting toward using synthetic CBD analogs.18 “Extensive first-pass metabolism and the observed polypharmacology of CBD make it challenging to relate its therapeutic effects to a precise molecular target. This complicates the optimization of compounds because no one target can effectively drive structure-activity relationship studies.”
They went on to say,” Synthetic analogues of CBD have been targeted based on modification of the C3-alkyl chain, the phenol ring, and the limonene moiety. Biological studies of these compounds led to identification of compounds with interesting pharmacological properties.”
In 2017, Russo provided a summary of the currently known benefits of CBD in an article in Trends in Pharmacological Sciences.5 He stated, “It [CBD] is a pharmacological agent of wondrous diversity, an absolute archetypal ‘dirty drug’, encompassing analgesic, anti-inflammatory, antioxidant, antiemetic, antianxiety, antipsychotic, anticonvulsant, and cytotoxic effects.”
Speaking to the complexity of mechanisms CBD may use, he added that its effects are “…mediated by a wide variety of signaling mechanisms including activity on cannabinoid receptors, 5-HT1A, GPR55, GPR18, TRPV1, and other transient receptor potential channels.”
In 2018, Jürg Gertsch at the University of Bern proposed that the placebo effect may play a role in the effects of cannabinoids like CBD.19 The “meaning response,” as he refers to it “may play a role in the broad palliative and therapeutic effects of medical cannabis unprecedented by other phytopharmaceuticals.” At the root of this hypothesis is, according to Nelson et al., the idea that “because CBD has been so conflated with cannabis, even if CBD has no direct pharmacological effect, its associated ‘meaning effect’ may activate a secondary pharmacological effect.”
Epidiolex is the only US Food and Drug Administration-approved drug containing CBD. It is used to treat two rare and severe forms of epilepsy known as Dravet syndrome and Lennox-Gastaut syndrome, in people two years of age and older.20 Epidiolex is administered as an oral solution containing 100 mg/mL of CBD.21
Dose Data
| Dose (mg/kg) | Administration | Species | Ref. | |
|---|---|---|---|---|
| LD50 | 50 | Intravenous | Mouse | 11 |
Receptor Binding Affinity Data
| Receptor | Ki (nM) | Species | Note | Ref. |
|---|---|---|---|---|
| CB1 | 4350 | Mouse | 12 | |
| CB2 | 2860 | Rat | 13 |